Abstract and Introduction
Purpose: The treatment options for viral myocarditis caused by coxsackievirus B are summarized.
Summary: Myocarditis is a common cause of dilated cardiomyopathy. The most common causes of infectious myocarditis are viruses. The exact mechanism of coxsackievirus B-induced damage to myocytes is unknown. The likely mechanisms involve immune-mediated and direct viral cytotoxicity. There are several proposed treatment strategies that target specific points in the pathway from myocarditis to cardiomyopathy. Immunosuppressive agents (azathioprine, prednisone, and cyclosporine) for the treatment of myocarditis seem logical, since one of the mechanisms thought to contribute to myocarditis is autoimmune destruction. Another treatment option of viral myocarditis is intravenous immunoglobulin (IVIG). As with conventional immunosuppressive strategies, IVIG suppresses the immune response. In addition, IVIG may replace antibodies, enhance viral clearance, neutralize pathogens, and enhance clearance of inflammatory cytokines that contribute to myocytes destruction. Antiviral agents, such as interferons, pleconaril, and acyclovir, target the causative organism, possibly halting the cascade of myocyte destruction. Natural products of particular interest in the treatment of viral myocarditis are Astragalus membranaceus and Ardisia chinensis. There is no specific therapy for patients with viral myocarditis or dilated cardiomyopathy. In general, patients with dilated cardiomyopathy will benefit from agents commonly used in heart failure, since their symptoms and presentation are similar.
Conclusion: Immunosuppressive agents, IVIG, antiviral agents, and natural medicines have been used in the treatment of patients with myocarditis. However, the efficacy of these agents has not been well established, partly because research has not differentiated between infectious and noninfectious myocarditis. This makes it difficult to extrapolate study results to viral myocarditis.
Myocarditis, or inflammation of the heart, is a common cause of dilated cardiomyopathy. Although most cases of myocarditis resolve spontaneously,[1] some cases result in dilated cardiomyopathy and subsequent symptomatic heart failure (HF), resulting in death for 50% of patients one to two years after diagnosis.[2,3] There is no specific treatment for myocarditis, except for the conventional treatment of HF symptoms, including heart transplantation. Approximately 45% of patients who undergo heart transplantation have underlying dilated cardiomyopathy.[4] The causes of myocarditis are commonly divided into three categories: infectious, toxic, and immunologic. Common causes of infectious myocarditis include viruses, parasites, protozoa, and fungi, with viruses being the most common cause.[4]
Coxsackieviruses are enteroviruses and are divided into two classes: A (composed of 23 serotypes) and B (consisting of 6 serotypes).[5,6] Coxsackievirus B is the most common viral culprit of myocarditis. In one study, 34% of patients with myocarditis and idiopathic dilated cardiomyopathy had enteroviral RNA present.[7] In addition, the mortality rate for patients with viral RNA was higher compared with patients in whom viral RNA was not present (25% versus 4%, p = 0.02). Hence, infection with coxsackievirus B may be an important indicator of patient outcome. Most adults have been infected with the virus at some point in their lives.[4] Why this virus produces severe effects in some and no effects in others is unknown. There is speculation that a genetic component may make some individuals more susceptible to the cardiotropic effects of coxsackievirus B.[6]
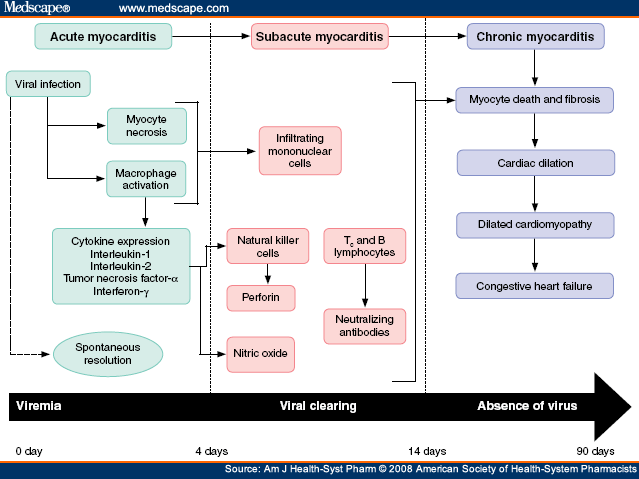
The exact mechanism of coxsackievirus B-induced damage to myocytes is unknown. The likely mechanisms involve immune-mediated and direct viral cytotoxicity.[4] Infected myocytes may express antigens that confound the immune system's ability to recognize the body's own myocytes, triggering an immune response. Natural killer (NK) cells, T lymphocytes, and other cells of the immune system are recruited in an attempt to clear the infectious agent. In addition, cytokines and other inflammatory mediators are released. NK cells recruited by the immune response to viral infiltration may have a cardioprotective effect by limiting viral replication but may also promote the release of perforin molecules, which destroy the integrity of the myocytes' cytoskeleton.[4] Cytokine release may contribute to the formation of excessive nitric oxide, which could lead to myocardial depression and cell death.[8] The combination of immune destruction and inflammatory response results in the necrosis of myocytes and subsequent replacement with fibrotic tissue. Whether dilated cardiomyopathy results from acute myocarditis or chronic myocarditis is still under debate.[9] Direct toxic effects of the coxsackievirus B may be amplified by malnutrition,[10] age, and exercise.[4] There has also been speculation that virus particles remain dormant in the myocardial tissue until a trigger causes reactivation and acute myocarditis.[9] Figure 1 outlines the postulated pathway from myocarditis to cardiomyopathy.[11,12,13]

The postulated pathways of the progression of myocarditis to cardiomyopathy. Adapted from references 11-13, with permission.
Am J Health Syst Pharm. 2008;65(2):132-137. © 2008 American Society of Health-System Pharmacists
Cite this: Treatment of Viral Myocarditis Caused by Coxsackievirus B - Medscape - Jan 15, 2008.


Comments