Introduction
Hypertension is a prevalent and independent promoter of vascular damage to the heart, brain, kidneys, and limbs. This condition afflicts about 50 million persons in the United States and as the population ages its prevalence is expected to increase. Long-term investigation of its occurrence in the Framingham Study indicates that 90% of persons who are normotensive at age 55 years can expect to develop hypertension in their lifetime. The cardiovascular risk it imposes varies in relation to the height of the blood pressure, which component is elevated, the target organ affected, and the burden of coexisting risk factors. Recent guidelines of the Seventh Joint National Committee on Hypertension (JNC 7) recommend consideration of more modest blood pressure elevations (i.e., prehypertension 120/80 mm Hg to 140/90 mm Hg) for some treatment. Efficient treatment of this lowered range of blood pressure elevation requires multivariable risk stratification of the so-defined hypertension to be cost-effective and avoid needlessly alarming patients.
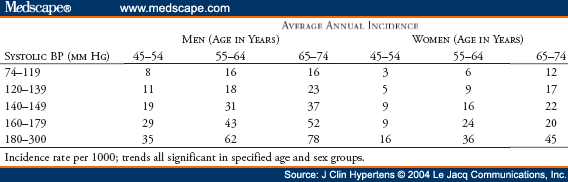
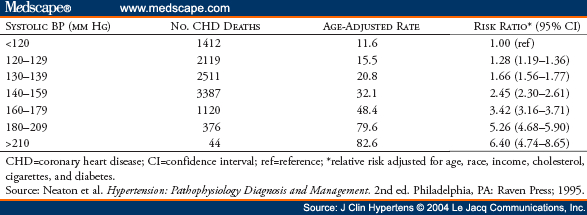
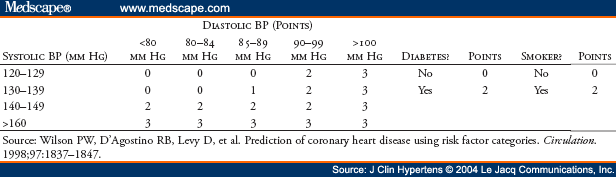
In 2003, a substantial amount of epidemiologic and clinical information was published concerning risk assessment of hypertension and its treatment. The JNC 7 guidelines for detection, evaluation, and treatment of elevated blood pressure specify, but do not quantify some of the criteria for risk assessment. The report emphasizes that systolic blood pressure is more important than diastolic blood pressure, citing an incremental cardiovascular disease (CVD) risk extending down to what was previously regarded as the normal range, defining a "prehypertensive" blood pressure category. Certain high-risk conditions like diabetes are designated "compelling indications" calling for more stringent blood pressure goals. A notable omission among these is dyslipidemia, a condition that should modify the blood pressure treatment goal because of its influence on hypertensive CVD risk.
© 2004 Le Jacq Communications, Inc.
Cite this: Hypertensive Risk Assessment: Cardiovascular Risk Factors and Hypertension - Medscape - Jul 01, 2004.